
There’s a particular kind of helplessness that comes when someone close to you receives a serious medical diagnosis. The doctors explain what it is, they write the prescription, and then you go home. In China, that’s usually where the process ends — you fill the medications, you follow the dosage instructions, and you trust that the hospital knows best.
I understood why that was the expectation. But this time, I couldn’t just accept it.
How It Started

The diagnosis had been coming for a while, even if we didn’t know what to call it. The tremor that showed up first in one hand. The gradual stiffening of movement. The way familiar tasks — buttoning a shirt, holding chopsticks steadily — started requiring visible effort. By the time we sat in the neurologist’s office and heard the word “Parkinson’s,” we had already been living with the reality for months without a name for it.
The doctor was thorough in his own way. He explained the disease mechanism briefly, wrote out a treatment plan — a combination of levodopa-based medication and an enzyme inhibitor to help the drugs work more effectively — and told us when to come back. The appointment was maybe twenty minutes. We left with two boxes of pills and a follow-up scheduled for three months later.
I went home and stared at the medication boxes on the table. I didn’t know what questions to ask, because I didn’t know enough to know what I didn’t know. That’s a strange kind of stuck.
The First Conversation I Should Have Had Earlier
I opened an AI chat and started asking basic questions. What actually happens in Parkinson’s disease? Why does dopamine matter? What does levodopa do, exactly, and why does it eventually stop working as well over time? What are the side effects we might see later, and how do caregivers usually manage them?
That conversation took about half an hour. By the end of it, I understood more about the disease than I had learned in three months of living with it. Not medical-school level — but enough to understand what the medication was doing, why the dosage would likely increase over time, and what symptoms would indicate that the current treatment was becoming less effective.
It sounds obvious in retrospect. Of course you should research a serious diagnosis. But the way Chinese patients are trained to relate to the medical system — trust the doctor, follow the prescription, don’t ask too many questions — makes it genuinely hard to know that more information is available and that you’re allowed to go find it.
The Search I Never Knew to Run
After the AI had helped me understand the basics, I asked a different question: what research is happening on this disease right now? Not “what is the current standard treatment” but “what is the frontier?”
The AI gave me a useful overview — stem cell therapies, adaptive deep brain stimulation, new drug candidates targeting alpha-synuclein. But I wanted something more concrete. So I wrote a short program to query ClinicalTrials.gov — the official global database for registered clinical trials — filtered specifically for Parkinson’s disease studies that were actively recruiting patients in China.
The result was 81 trials.
I sat with that number for a moment. I don’t know what I expected — five, maybe, or ten. A small list I could quickly exhaust. Instead I was looking at 81 active studies, many of them recruiting right now, at hospitals I could actually reach. I’ve used AI for a lot of things over the past two years — writing, investing research, building side hustles. But I don’t think I’ve ever felt the way I felt in that moment. Not excited, exactly. Something quieter. Like a door had opened that I didn’t know existed, in a hallway I thought I already knew by heart.
I had prepared myself for the answer that “there isn’t much happening.” Instead, I was looking at a list of ongoing research across dozens of hospitals — Beijing Tiantan Hospital, Ruijin Hospital in Shanghai, Xuanwu Hospital, West China Hospital in Chengdu. Trials covering brain stimulation, new drug formulations, traditional medicine approaches, early detection biomarkers, and — the one that stopped me — cell therapy.
The Part That Changed How I Think About This
Among the 81 trials were several studying iPSC-derived dopaminergic neurons — a technology where induced pluripotent stem cells are used to grow new dopamine-producing neurons that can be transplanted into the brain. The idea is not to manage symptoms but to restore the cells that Parkinson’s destroys.
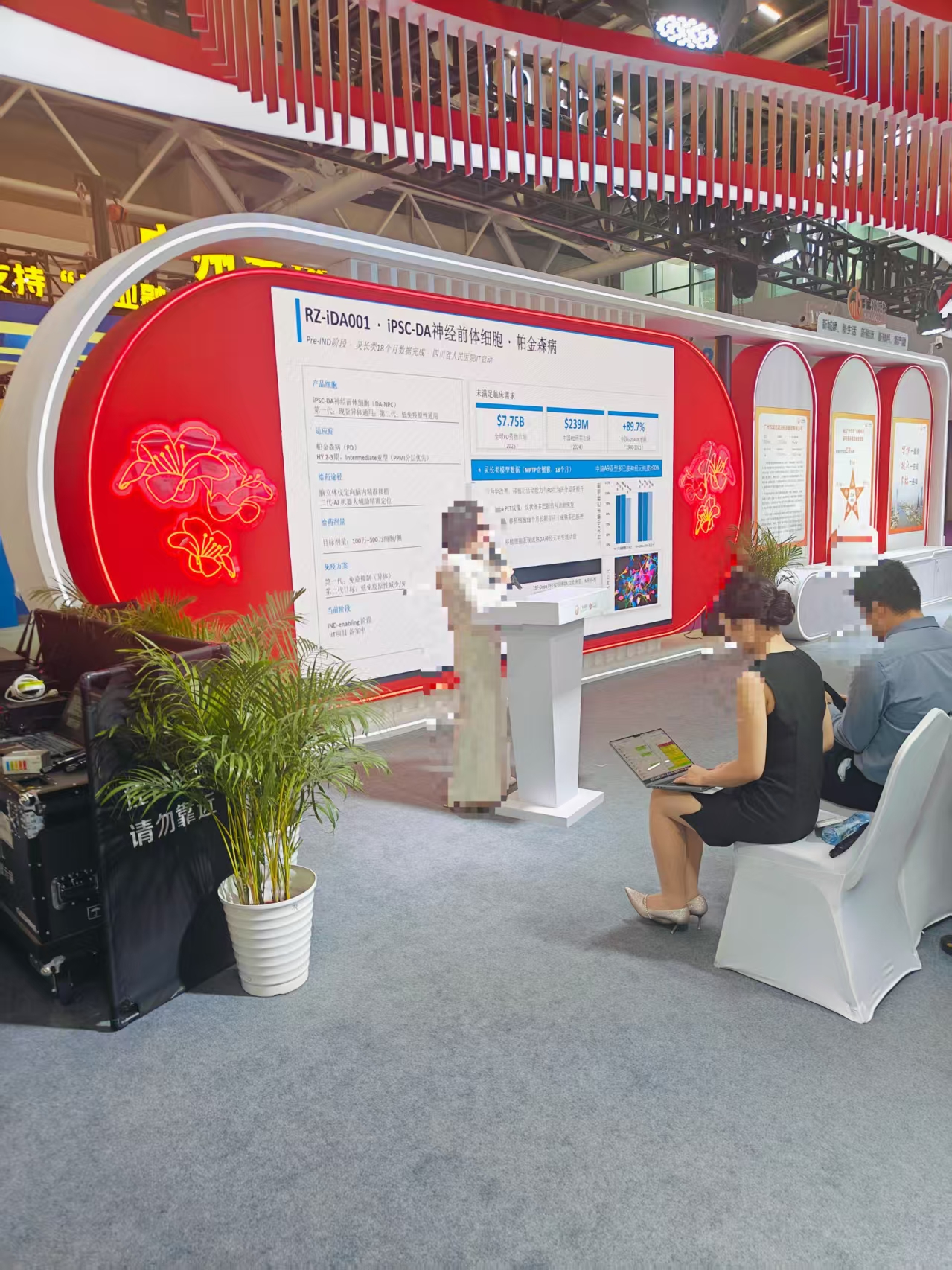
Around the same time, I came across a conference presentation on exactly this technology — researchers showing early data on iPSC-based neural transplantation, tracking outcomes, presenting phase data. Seeing it presented seriously, by credible institutions, at a real conference, made the clinical trial entries in my list feel less abstract.
This is not science fiction. There are Phase 1 trials running right now in Chinese hospitals testing whether this approach is safe. Roche has a Phase 3 trial (Prasinezumab) actively recruiting at 20 sites across China. Medtronic is running an adaptive deep brain stimulation study at five major hospitals simultaneously — a technology that adjusts its stimulation in real time based on what the brain is actually doing, rather than a fixed setting.
None of this appeared in any of the conversations we’d had with the hospital. Not because doctors were hiding it — they weren’t — but because a fifteen-minute appointment isn’t the right venue for a survey of the global research landscape. That’s not what those appointments are for.
What I Built After
Once I understood the landscape, I built a simple home observation log — a structured form for recording daily symptoms, medication timing, sleep quality, and any changes in motor or cognitive function. Not because I expected to become a clinician. But for two reasons: first, if we ever do pursue a clinical trial, that kind of systematic record is exactly what enrollment teams ask for. Second, because paying close attention is itself a form of care. Having a structured way to observe meant I stopped passively worrying and started doing something concrete.
I also set up an automated monitor on the ClinicalTrials database, so if new Parkinson’s trials open up in China, I’ll know about them.
What AI Actually Did Here
It didn’t give me hope in some vague, motivational way. It gave me specific, actionable information that I couldn’t have found on my own in any reasonable amount of time.
The doctors manage the medical care. That’s their job and they do it. What AI did was help me move from passive observer to informed participant — someone who understands the treatment landscape, knows what research exists, and can ask better questions at the next appointment.
For a disease that most people accept as a one-way door, finding out that dozens of research teams across China are actively working on it — some of them on approaches that could fundamentally change the trajectory — felt like something worth knowing.
I’m not sure that counts as hope, exactly. But it felt like the opposite of helplessness.
Frequently Asked Questions
How do I search for Parkinson’s disease clinical trials in China? The most reliable source is ClinicalTrials.gov — the official global registry maintained by the U.S. National Library of Medicine. You can filter by condition (“Parkinson Disease”), status (“Recruiting”), and location (“China”). As of mid-2026, there are over 80 actively recruiting trials. Major research centers include Beijing Tiantan Hospital, Xuanwu Hospital, Ruijin Hospital in Shanghai, and West China Hospital in Chengdu.
What is iPSC therapy for Parkinson’s disease? iPSC stands for induced pluripotent stem cells. Researchers take a patient’s own cells, reprogram them into stem cells, then guide them to develop into dopamine-producing neurons — the exact type of cell that Parkinson’s destroys. These neurons are then transplanted into the brain. The goal is not to manage symptoms but to restore the lost cells. Several Phase 1 trials testing the safety of this approach are currently running in China.
What medications are typically prescribed for Parkinson’s disease in China? The standard first-line treatment is levodopa, most commonly combined with benserazide (sold under the brand name Madopar, manufactured by Roche). As the disease progresses, doctors often add entacapone — a COMT inhibitor that slows the breakdown of dopamine and extends the effectiveness of each levodopa dose. These are the same medications used as first-line treatment globally.
Can AI replace a doctor for Parkinson’s disease research? No — and that’s not what it’s for. AI is useful for helping a non-specialist understand a complex landscape: how the disease works, what research exists, which clinical trials are recruiting, and what questions are worth asking at the next appointment. The medical decisions themselves still belong to the treating physician. What AI changes is the quality of the conversation you can have with that physician.
Have you ever used AI to research a medical situation — for yourself or someone close to you? What did you find that surprised you?
Share your experience or thoughts below.
Related Reading
- My Friend Is 45 and Works in IT. He Asked Me What to Do. I Asked AI. Here’s the Roadmap.
- I Spent ¥340 on a Mini PC to Run a Local AI Agent. The AI Chose the Hardware. The Software Was Already Obsolete.
- My Dad Said “Just Use the AC.” I Asked AI Instead. ¥546 Later, I Barely Need It.
Free Tools From This Blog
Leave a Reply